
Overview
 Morton?s Neuroma is a pain condition that affects your feet and toes. If you are suffering from Morton?s Neuroma, a growth of tissue has developed over one of the nerves running from your feet into your toes. This growth can cause inflammation and pain whenever you use your foot. A type of benign tumor, Morton?s Neuroma typically develops in the space between the third and fourth toes, although it can also form between the second and third toes. When you walk, the bones and ligaments in the top of your foot press down on this growth, causing pressure and pain.
Morton?s Neuroma is a pain condition that affects your feet and toes. If you are suffering from Morton?s Neuroma, a growth of tissue has developed over one of the nerves running from your feet into your toes. This growth can cause inflammation and pain whenever you use your foot. A type of benign tumor, Morton?s Neuroma typically develops in the space between the third and fourth toes, although it can also form between the second and third toes. When you walk, the bones and ligaments in the top of your foot press down on this growth, causing pressure and pain.
Causes
Morton’s Neuroma is a caused by pressure, abnormal function/motion or an imbalance in the structure of the foot such as flat feet, that causes an abnormal pressure on the structures and the nerves in the ball of the foot. It most commonly affects the nerve that goes to the 2nd 3rd or 4th toes. The squeezing of the nerve from abnormal motion leads to a protective thickening of the sheath that protects the nerve. Symptoms of Morton’s Neuroma often occur during or after activities that cause a sidewards squeezing of the ball of the foot or from pressure such as walking, standing, or playing sport. Since squeezing is a common cause of the condition, shoes such as pointed toes or high heels can often lead to a neuroma. Shoes that are constricting, even tight sneakers, can pinch the nerve between the toes, causing inflammation and pain.
Symptoms
If you have a Morton?s neuroma, you may have one or more of these symptoms where the nerve damage is occurring, Tingling, burning, or numbness, pain, a feeling that something is inside the ball of the foot or a feeling that there?s something in the shoe or a sock is bunched up. The progression of a Morton?s neuroma often follows the following pattern. The symptoms begin gradually. At first they occur only occasionally, when wearing narrow-toed shoes or performing certain aggravating activities. The symptoms may go away temporarily by removing the shoe, massaging the foot, or by avoiding aggravating shoes or activities. Over time the symptoms progressively worsen and may persist for several days or weeks. The symptoms become more intense as the neuroma enlarges and the temporary changes in the nerve become permanent.
Diagnosis
The diagnosis of interdigital neuroma is usually made by physical examination and review of the patient’s medical history.MRI ad High Definition Ultrasound examination may be useful to confirm the diagnoses however they may still not be 100% reliable. The commonest reason for this is de to natural substances present in between the metatarsal heads and between the fat pad and the intermetatarsal ligament. These natural substances i.e. bursa, fat, capsular thickening and even bony growths, can all be a factor in the impingement process and may need to be surgically cleared.
Non Surgical Treatment
Conservative treatment involves a reduction in the inflammation and removing the impingement factor. Reduction in inflammation is achieved via rest, elevation, ice, and massage with anti-inflammatory gels. Removing foot wear and and/r wearing broad type footwear would also help. Injection therapy is useful in reducing symptoms but not very successful in providing long term relief. The only time when it is most appropriate is when the cause of the space occupying object is not a neuroma but an inflamed bursa. Injection would help to relieve symptoms, and often cortisone is not even necessary.
Surgical Treatment
For severe or persistent pain, you may need surgery to remove the neuroma. Once the nerve is gone, you permanently lose feeling in the affected area. One alternative to surgery is to undergo neurolysis injections. These use chemical agents to block pain signals. Another alternative is to take a prescription pain reliever that alleviates nerve pain.




 Overview
Overview Symptoms
Symptoms
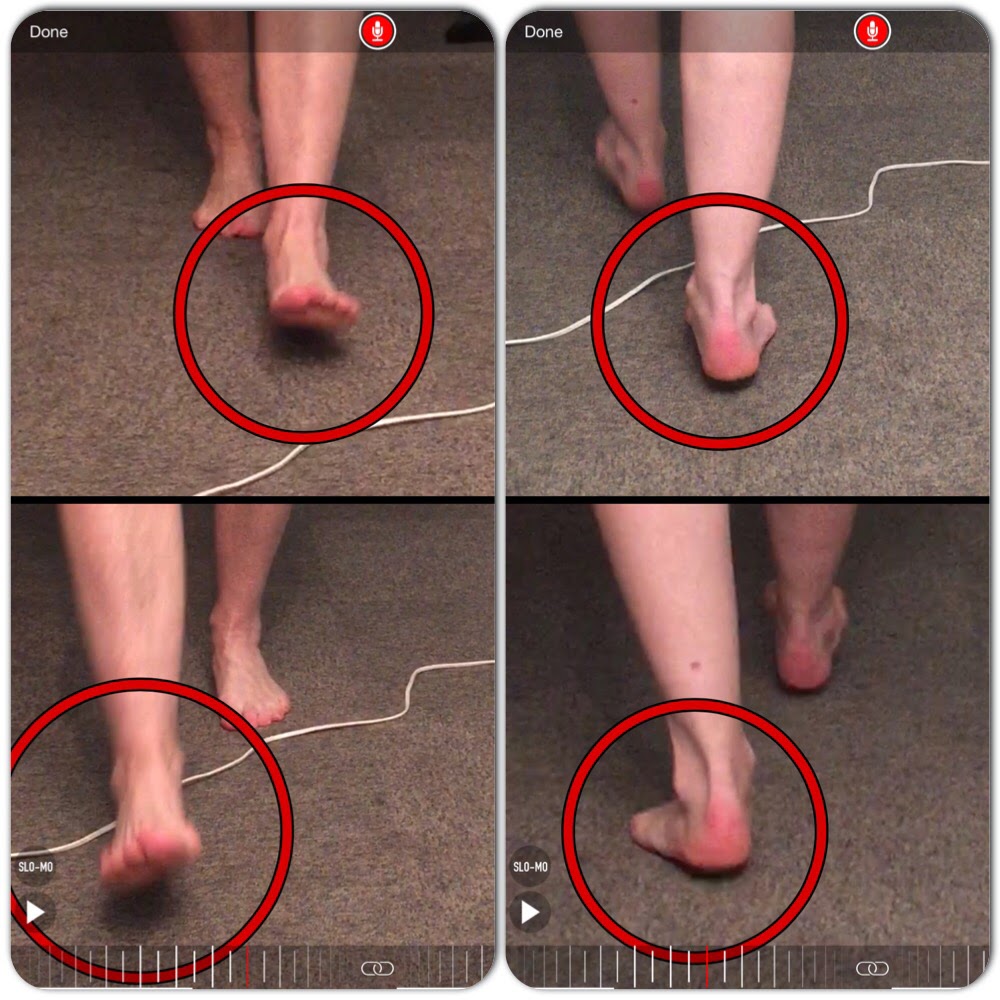



 The Achilles tendon is the thickest and strongest tendon in your body, connecting your calf muscles to the back of your heel. Virtually all of the force generated when you ?toe off? the ground during running is transmitted by the Achilles, and this force can be as much as three times your body weight. And the faster you run, the more strain you put on the Achilles tendon. As such, it?s prone to injury in many runners, but particularly those who do a lot of fast training, uphill running, or use a forefoot-striking style. Achilles tendon injuries account for 5-12% of all running injuries, and occur disproportionately in men. This may be because of the faster absolute speeds men tend to train at, or may be due to other biomechanical factors.
The Achilles tendon is the thickest and strongest tendon in your body, connecting your calf muscles to the back of your heel. Virtually all of the force generated when you ?toe off? the ground during running is transmitted by the Achilles, and this force can be as much as three times your body weight. And the faster you run, the more strain you put on the Achilles tendon. As such, it?s prone to injury in many runners, but particularly those who do a lot of fast training, uphill running, or use a forefoot-striking style. Achilles tendon injuries account for 5-12% of all running injuries, and occur disproportionately in men. This may be because of the faster absolute speeds men tend to train at, or may be due to other biomechanical factors.

You must be logged in to post a comment.